FIGURE 1 Mental health Uniform Crime Reporting-coded call data overview.
| Journal of Community Safety and Well-Being (2026) 11(1), 17–25. | https://doi.org/10.35502/jcswb.504 |
Madison Charman∗
This article is related directly to the Seventh International Conference on Law Enforcement & Public Health (LEPH) held in Ottawa, Canada in July 2025.
ABSTRACT
Police services across Canada are increasingly responding to mental health-related calls that stem from social and health challenges rather than criminal behaviour. Despite the availability of crisis lines and community-based mental health resources, many of these calls continue to be routed through police dispatch. This paper presents a data-informed case study from the Barrie Police Service, analyzing over 1,400 calls for service using Uniform Crime Reporting codes, Records Management System entries, and Computer-Aided Dispatch data. The findings reveal that the majority of mental health-related calls are non-criminal, non-reportable, and do not result in apprehensions or charges. Notably, there were discrepancies between how calls were initially reported and how they were later classified, with only one-third originally categorized as Mental Health Act related. Call priority data further revealed that just 1% of mental health calls indicated an immediate safety concern, while 44% were classified as moderate safety risks. The remaining 55% of calls did not present significant safety threats, suggesting they could be more appropriately handled by non-police, community-based response teams. These results challenge prevailing narratives that equate mental illness with risk and harm, and they highlight the need for upstream, community-based interventions tailored to individuals with repeated police interactions.
Keywords Police, mental health, alternative response, law enforcement and public health conference.
Police across Canada are increasingly responding to incidents rooted in social disorder and health-related crises (Cotton & Coleman, 2014 Fahim et al., 2016). Many of these calls, particularly those involving mental health, fall outside the scope of traditional criminal enforcement. This growing trend raises important questions about the role of police in managing mental health-related calls for service, especially when the majority do not involve criminal behaviour or require a conventional law enforcement response. Multiple studies have sought to identify and evaluate police responses to persons experiencing and/or living with mental illness, including the prevalence of mental health concerns among individuals who interact with police and the development of specialized intervention models (El-Sabawi & Carroll, 2021; Shapiro et al., 2015). However, few have conducted in-depth analyses of police data to assess the actual necessity of police involvement in these calls. There remains limited empirical evidence regarding the actual nature of these calls and the extent to which they require police-specific intervention. Additionally, literature is still unclear on whether individuals experiencing mental health challenges are more likely to engage in violent behaviour (Ahonen et al., 2019; Choe et al., 2008; Elbogen & Johnson, 2009).
In-depth analysis of police data itself on interactions and outcomes of calls with individuals experiencing mental health crises remains limited, in part due to the risk-averse nature of police organizations and a general reluctance to share internal data. This study seeks to address that gap by providing a transparent, data-driven examination of mental health-related calls for service within a mid-sized Canadian police agency. While police data offer an important starting point for understanding mental health-related calls, particularly when exploring the feasibility of alternative response models, it is important to acknowledge the limitations inherent in these data. Police data can lack consistency in how mental health information is coded or categorized, and can also be difficult to extract mental health components from general call data (Boyce et al., 2015; Huey et al., 2021; Sinha, 2009).
Since the deinstitutionalization era, police have increasingly become the default responders to individuals with mental health needs (Wood et al., 2011). With community supports often unable to meet growing demand, many individuals face ongoing challenges such as unstable housing, substance use, limited access to treatment, and persistent stigma (Theuer, 2024). These gaps led to the reinstitutionalization of individuals with mental health challenges via the criminal justice system, with police frequently called due to perceived danger or unpredictability (Dempsey et al., 2020; Lamb et al., 2004). This shift contributed to the criminalization of mental illness, as individuals were more likely to be charged or apprehended to resolve calls. As a result, police officers became “de facto mental health professionals,” prompting the development of specialized response models such as co-response teams (e.g., mobile crisis intervention teams), and police-led internal units with crisis intervention training (Coleman & Cotton, 2016; Compton et al., 2014; Davis et al., 2025; El-Sabawi & Carroll, 2021; Shapiro et al., 2015).
Alternative crisis response models are rapidly gaining municipal adoption to address mental health-related calls historically routed to law enforcement. Operational models vary by jurisdiction: the City of Barrie’s Community Alternative Response Engagement (CARE) Team is a multi-agency partnership that leverages existing Barrie Police Service communicators to divert appropriate mental health calls. Conversely, the Toronto Community Crisis Service (TCCS) is a non-police, community-based mobile response for mental health and wellness checks, primarily dispatched via 211 (City of Toronto, n.d.). US programs include Denver’s Support Team Assisted Response (STAR) program, which pairs behavioural health clinicians with paramedics (City of Denver, n.d.). Similarly, Durham, North Carolina’s Holistic Empathetic Assistance Response Team (HEART), a non-police unit within the city’s Community Safety Department, dispatches unarmed, three-person teams to non-violent 911 calls (City of Durham, n.d.). These teams are typically composed of a mental health clinician, a peer support specialist, and an emergency medical technician. Eugene, Oregon’s Crisis Assistance Helping Out on the Streets (CAHOOTS) program was a pivotal early model for these efforts. Unfortunately, CAHOOTS announced that it is no longer available, and the city is now served by a county-level mobile crisis response team (City of Eugene, 2025).
The goal of non-police response teams is to reduce police involvement in mental health calls when appropriate. However, the primary resistance to adoption is rooted in the perceived operational risk and safety of alternative first responders (Atherley, 2025; Ratcliffe, 2021). This is also heavily seen in the dispatching level of non-police teams where communicators act as gatekeepers, deciding whether to divert a call away from a guaranteed armed police response to an unarmed civilian team. Dispatchers report intense anxiety over personal and jurisdictional liability if they send a crisis team and the incident escalates rapidly into violence or involves an unexpected threat (Thompson, 2024). This challenge is summarized by Ratcliffe’s Paradox (2021), which posits that the information needed to safely discriminate and divert a public health call is lacking at the dispatch level; paradoxically, it often requires an initial in-person assessment by an all-hazards responder (police) to confirm the situation is safe enough for a specialist non-police team. This structural problem is amplified by policing’s inherent, highly risk-averse posture, which Atherley (2025) suggests leads to the catastrophizing of rare risks – like the occasional, tragic violence against responders – making dispatchers default to the police blanket approach. Critically, this hesitation is mirrored by the public, as Addison et al. (2023) found that three-quarters (76.6%) of the community surveyed agreed that police are needed during a mental health crisis for safety reasons.
Despite the concerns about safety and liability, the track record of established non-police response teams demonstrates a remarkably low rate of escalation requiring police involvement. For example, the pioneering CAHOOTS model, operating in Eugene, Oregon, since 1989, requires police backup in only 1% of its calls. Denver’s STAR program reported an even stronger safety record, having never called for police backup due to a safety issue as of July 2022. Similarly, in Durham, members of the HEART reported feeling safe in an overwhelming majority (99%) of calls. The TCCS, which handled 5,860 events in its first year (2023), workers specifically requested police backup only 100 times, translating to a backup rate of approximately 1.7% (Centre for Addiction and Mental Health, 2023). These consistent, low reliance rates across varied models and geographies strongly indicate that the perceived operational risk of non-police response is far greater than the actual risk. Barrie’s CARE Team data on police co-response is not publicly available.
The fundamental disconnect between organizational and public anxiety and the proven safety records of non-police teams highlights a critical need for rigorous, local data. This tension is encapsulated by Atherley’s question: “Although ‘opportunity’ for a non-police response appears significant, particularly with the aid of hindsight, what is the ‘opportunity cost’?” (p. 2). This study aims to quantify that cost by analyzing the actual safety risk in mental health calls and the feasibility of deploying non-police teams safely in a mid-sized urban setting. This retrospective observational study provides a comprehensive, data-driven analysis of 1,414 mental health-related calls for service received by the Barrie Police Service in 2024. Drawing on both Computer-Aided Dispatch (CAD) records and Uniform Crime Reporting (UCR) data, the research systematically examines the scope and characteristics of these calls, the nature of police involvement, and the roles of individuals involved. By investigating the intersection between mental health crises and criminal justice involvement, this analysis aims to directly inform ongoing discussions about the appropriateness of police-led responses and the potential for alternative, health-led approaches.
The analysis is guided by the following research questions (RQs):
Together, these questions aim to inform a more evidence-based approach to police response, resource allocation, and diversion strategies in addressing mental health in the community. The findings carry important implications for public safety policy, mental health service delivery, and the evolving role of police in responding to individuals in crisis.
This study was conducted in Barrie, Ontario. The City of Barrie has a population of approximately 150,000 (Statistics Canada, 2024). The community is served by the Barrie Police Service, comprising roughly 250 sworn officers and 130 civilian staff (Barrie Police Service, 2025). The city features a dense downtown core that hosts a concentration of social services, surrounded by suburban residential areas. It is well connected to the Greater Toronto Area via a major highway and commuter rail service. The city also contains a regional hospital that provides healthcare services to both urban residents and the surrounding rural population, as well as a post-secondary institution that contributes to the local economy and workforce development.
This study draws on administrative data collected by the Barrie Police Service, focusing specifically on mental health-related calls for service between 2019 and 2024. The primary call for service volume and initial incident categorization data utilized in this study are sourced directly from the Barrie Police Service’s CAD system. CAD records capture the total volume of mental health-related calls for service, alongside key initial classification metrics. These data reflect the instantaneous decision-making environment of the dispatch centre, as CAD data capture the initial classification of calls as described by the public and interpreted by police communicators at the time of dispatch. This initial categorization, and the priority level assigned by the dispatcher, is a critical input for understanding the perceived risk that governs the subsequent police response. In 2024, there were a total of 76,345 calls for service. Of those, 764 were classified as a mental health call in CAD by Barrie Police Service communicators.
These data are then downloaded into the Records Management System (RMS) and given context-specific UCR codes by records clerks. UCR coding attached to call data reflects validated and finalized classifications entered by officers or records management units following the completion of an investigation or incident report. These data are considered more accurate for analytical purposes, as they provide a standardized, post hoc view of police occurrences. The UCR code used for this analysis was “8529 – Mental Health Act (MHA).” Under this code are varying subcodes such as 8529.0110 – Attempt Suicide and 8529.0150 – Apprehension. All subcodes are included in the count of the master 8529 MHA master code. In 2024, there were 1,141 calls with the mental health UCR code 8529. Again, this is higher than the original 764 classified by communicators. Additionally, there were 81,327 calls recorded in the Niche RMS. This is higher than CAD calls as it also includes online reports that do not go through our CAD system. There are more calls with UCR codes of mental health than CAD-categorized mental health calls. This is because UCR coding is done upon the completion of the call with all the facts gathered, rather than an initial assessment based on information provided by the caller. This paper, therefore, will analyze calls for service with a UCR code of MHA (8529) rather than CAD mental health call classifications as the cohort of mental health calls; however, CAD classification discrepancies will also be further discussed.
Calls coded with a mental health UCR code linked back to their corresponding CAD records, enabling comparison between initial dispatch classifications and final determinations. Variables included whether the call resulted in a police report, criminal charges, or apprehension under the MHA. Where available, individual-level data were used to assess patterns of repeat contact, charges, or harm over time. The analysis employed descriptive statistics, case classification, outcome tracking, and a simple regression to explore trends in call volume, outcomes, and resource allocation related to mental health responses.
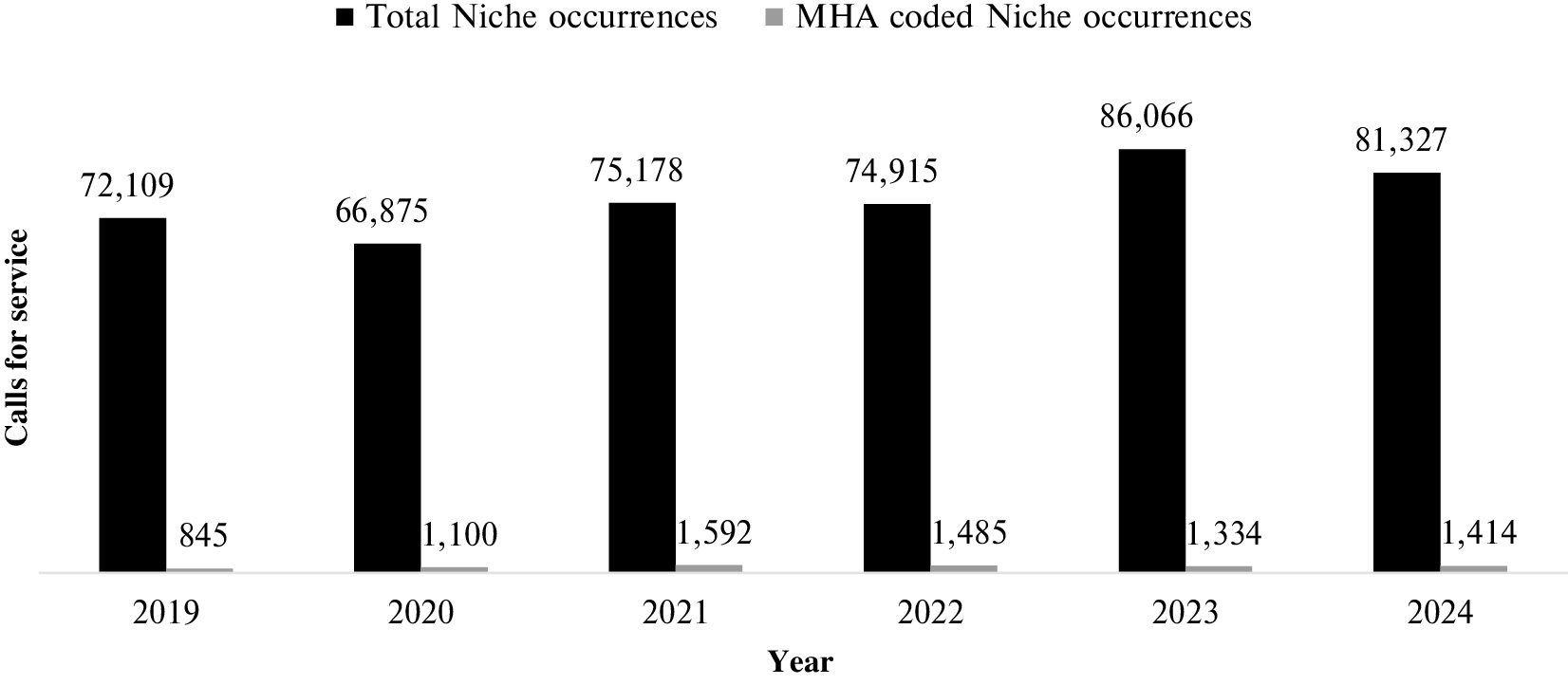
The first RQ aims to understand the volume and trends in mental health calls to police. An analysis of police call data from the Barrie Police Service highlights a growing demand for mental health-related responses. Between 2019 and 2024, the number of calls for service coded as mental health (8529) rose from 845 to 1,414, which demonstrates an increase of approximately 67%. While total police calls fluctuated during this period, ranging from 66,875 in 2020 to a peak of 86,066 in 2023, the proportion of calls related to mental health steadily increased (see Figure 1). In 2019, MHA-related calls accounted for 1.17% of all calls; by 2024, that figure had risen to 1.74%. The general MHA UCR is further broken down into subcodes shown in Table I.
|
|
||
|
FIGURE 1 Mental health Uniform Crime Reporting-coded call data overview. | ||
TABLE I Mental health UCR code and subcodes (2024)
| UCR Code | 2024 Calls | Proportion of Mental Health | Proportion of Total Calls |
|---|---|---|---|
| MHA (Master Code) | 499 | 35.29% | 0.61% |
| MHA – Apprehension | 636 | 44.98% | 0.78% |
| MHA – Attempt Suicide | 95 | 6.72% | 0.12% |
| MHA – Health Care Consent Act | 190 | 13.44% | 0.23% |
| MHA – No Contact With Police | 46 | 3.25% | 0.06% |
| MHA – Placed on Form | 326 | 23.06% | 0.40% |
| MHA – Threat of Suicide | 276 | 19.52% | 0.34% |
| MHA – Voluntary Transport | 44 | 3.11% | 0.05% |
| Total MHA | 1,414 | 100% | 100% |
MHA = Mental Health Act; UCR = Uniform Crime Reporting.
To assess whether this increase reflects a statistically meaningful trend over time, a simple linear regression was conducted with year as the independent variable and MHA-coded occurrence volume as the dependent variable. A simple linear regression analysis was used to test if the passage of time (in years) significantly predicted the annual volume of mental health-related calls. The results of the regression indicated the predictor explained 44% of the variance (R2 = 0.44, F(1, 4) = 3.20; p = 0.15). It was found that time did not significantly predict the annual volume of calls (β = 98.29; p = 0.15). Another simple linear regression analysis was used to test if the passage of time (in years) significantly predicted the annual proportion of mental health-related calls. The results of the regression indicated the predictor explained 14.9% of the variance (R2 = 0.15, F(1, 4) = 0.69; p = 0.45). It was found that time did not significantly predict the annual proportion of MHA-coded calls (β = 0.069; p = 0.45).
Call source
In 2024, 51% of mental health UCR-coded calls for service (n = 1,414) originated from the non-emergency police line, while 46% were initiated through 911. A small proportion of calls (2%) were proactively generated by officers, and 1% resulted from in-person walk-ins to the station. These findings suggest that most mental health calls enter the system through non-emergency reporting.
Call types and prevalence
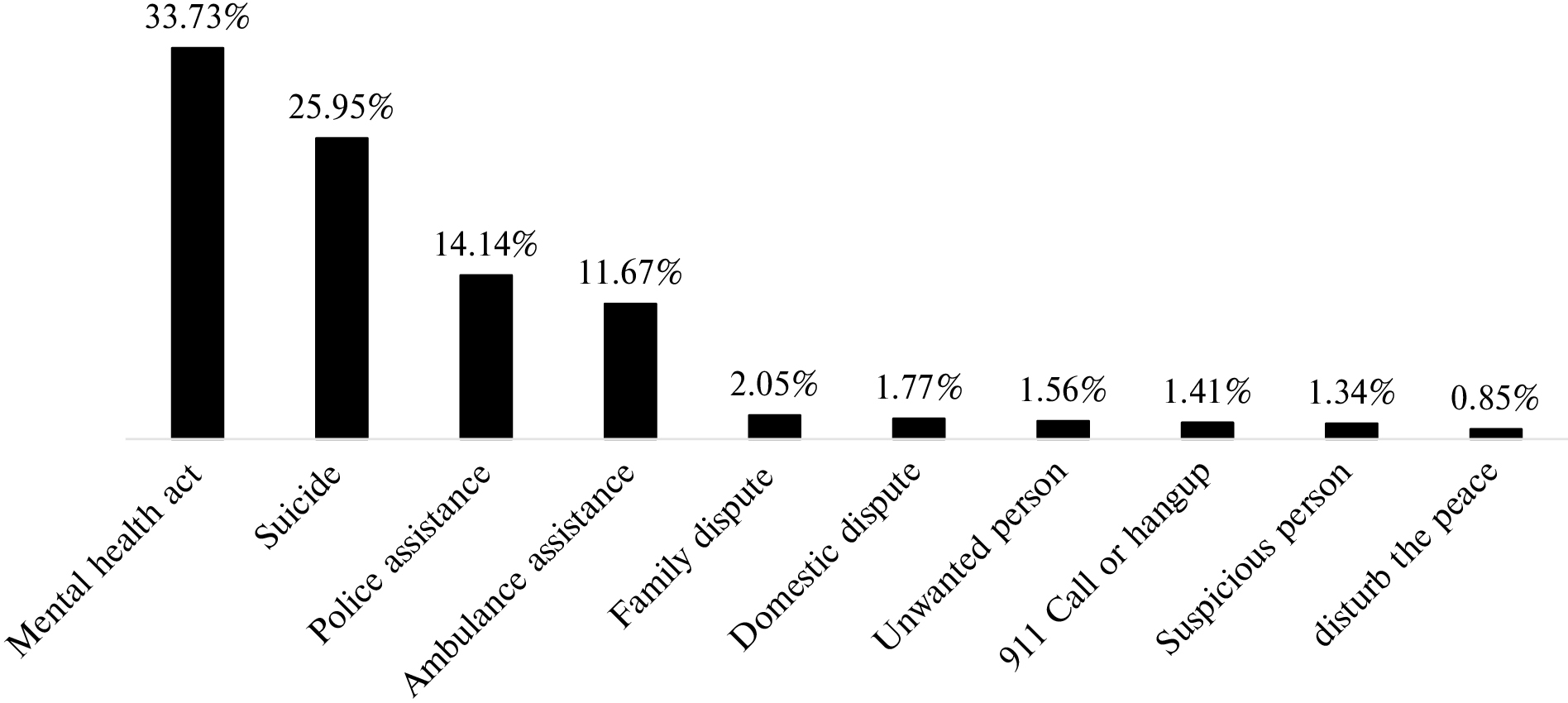
Significant discrepancies were found between how mental health-related calls were initially reported and how they were later classified. Of the 1,414 calls UCR coded as mental health calls (8529), 33.73% (n = 477) were originally coded as “MHA” in the CAD system. CAD classifications reflect how events are first conveyed by callers and interpreted by police communicators, highlighting a gap between initial perceptions and final categorization. The next most common was “Suicide,” accounting for 25.95% (n = 367) of cases. Other frequent classifications included “Police Assistance” (14.14%, n = 200), “Ambulance Assistance” (11.67%, n = 165), “Family Dispute” (2.05%, n = 29), “Domestic Dispute” (1.77%, n = 25), and “Unwanted Person” (1.56%, n = 22).
Call priority
To gain a clearer understanding of safety concerns associated with mental health-related calls, dispatch priority levels were used as an indicator of perceived risk. The Barrie Police Service categorizes calls for service into five priority levels based on urgency and risk. Priority 0 is the highest level, reserved for emergencies involving an immediate threat to life or serious harm (e.g., violent crimes in progress or major hazards). These calls require an immediate, two-officer response, with all available resources redirected if necessary. Priority 1 calls are urgent but slightly less critical, involving moderate threats such as ongoing property crimes or suspects fleeing the scene. These also typically require a two-officer response, with resources reallocated promptly. Priority 2 represents moderate-priority calls where the threat to safety is minimal, and suspects are no longer on scene; these usually warrant a single officer and may be delayed if higher priorities exist. Priority 3 includes routine or follow-up calls with no immediate threat, often handled by non-front-line police responses (such as online or phone alternative response officers) or scheduled at the convenience of the officer. Finally, priority 4 is reserved for proactive or administrative duties, carried out when no active service calls are pending. In all cases, responses are adapted based on unit availability, supervisor discretion, and evolving call circumstances. While this is not always as clear-cut in responses and real life, it is the most quantifiable indicator of risk available.
CAD priority data for the mental health UCR calls (n = 1,414) are displayed in Table II. The data show that 1% of the mental health calls were considered priority 0, meaning there was a significant safety concern. Additionally, 44% of mental health calls were considered priority 1, indicating a moderate safety threat. Therefore, 45% of mental health calls demonstrated a safety concern and may not be appropriate for alternative responses. In contrast, 55% did not demonstrate significant safety concerns.
TABLE II Mental health UCR-coded calls by priority (2024)
| Priority | Niche MHA Occurrences | Percentage |
|---|---|---|
| Priority 0 (high threat of serious physical harm) | 11 | 1% |
| Priority 1 (moderate threat of serious physical harm) | 624 | 44% |
| Priority 2 (minimal threat of serious physical harm) | 383 | 27% |
| Priority 3 (no threat of physical harm) | 292 | 21% |
| Priority 4 (no threat of physical harm) | 102 | 7% |
| Missing data | 2 | 0% |
| Total calls | 1,414 | 100% |
MHA = Mental Health Act; UCR = Uniform Crime Reporting.
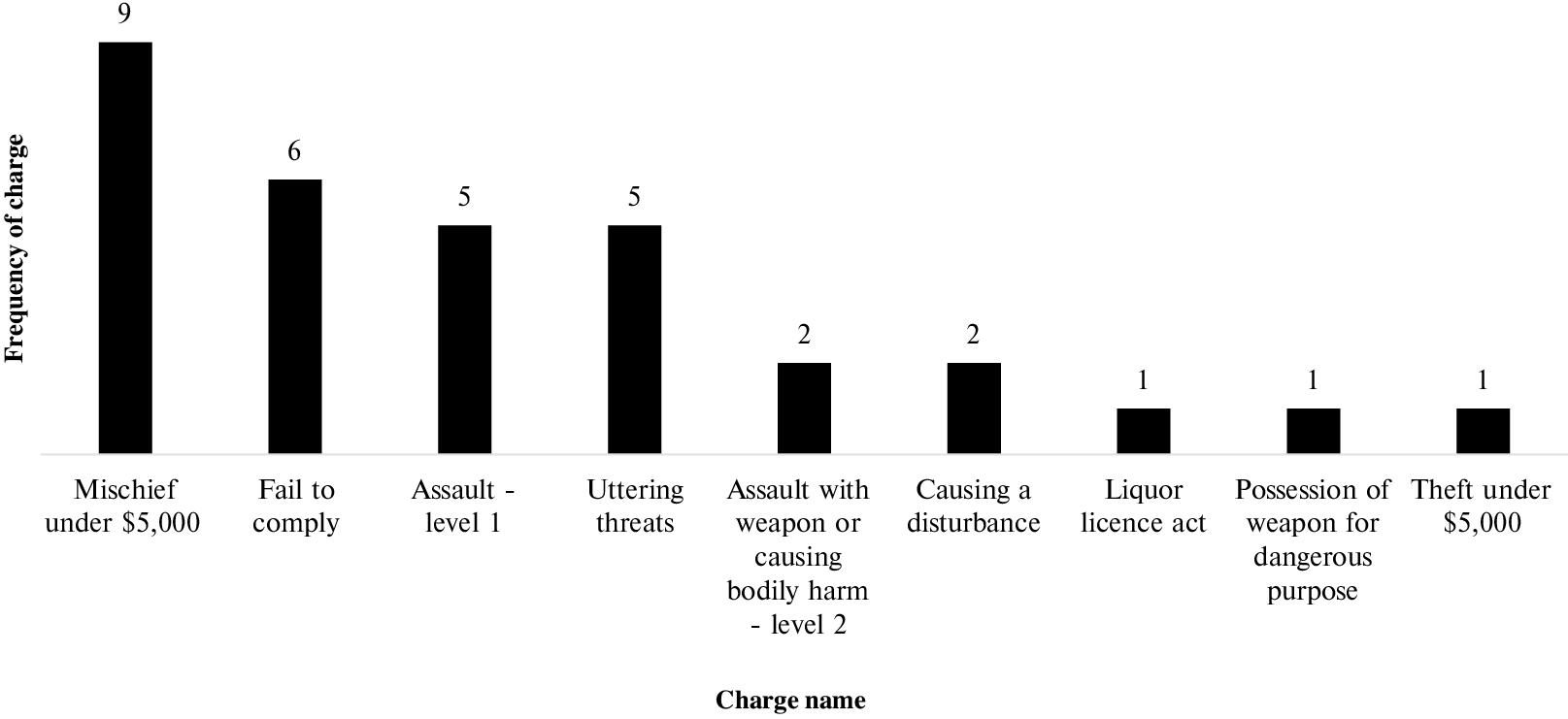
Of the 1,414 MHA-coded calls examined, the vast majority were resolved without the identification of a criminal offence. Specifically, 1,330 calls (94.06%) were cleared as “complete – solved (non-criminal),” while an additional 32 calls (2.26%) were marked as “complete – unsolved (non-criminal).” Only 18 calls (1.27%) resulted in criminal or recommended charges. These calls resulted in 32 criminal charges total, as displayed in Figure 2.
|
|
||
|
FIGURE 2 Resulting criminal charges in mental health-coded (8529) calls (2024). | ||
The most frequently identified offences in this group were level 1 assault, mischief, and uttering threats. These incidents involved a total of eight victims. Their relationship to the charged person included intimate partner (n = 2), hospital security (n = 2), neighbour (n = 2), parent (n = 1), and first responder (n = 1). The remaining clearances resulted in a variety of non-criminal outcomes.
Analysis of the data reveals a highly concentrated pattern of individual involvement within mental health calls. This is common among criminological scholarship, noting that a small number of people are often responsible for a high level of incidents or interactions (Sherman, 2007). This is often referred to as the “power few,” and in other disciplines as a power-law or Pareto distribution. A power-law distribution was observed in the context of mental health policing: just 4% of the individuals who initiated or were involved in mental health calls were linked to a total of 20% of the recorded calls. This significant overrepresentation points directly to a small cohort of high-frequency users who are experiencing chronic mental health crises, often compounded by complex, unmet social needs.
Finally, to address the intersection between mental health crisis and criminal justice involvement, data on individuals who were charged with a criminal offence were analyzed. The core purpose of this analysis is twofold: to empirically evaluate the actual safety risk posed by individuals during mental health-related calls and to identify patterns of chronic justice system entanglement that may fuel institutional risk aversion. Specifically, we examined whether individuals involved in a mental health-related call were also subject to criminal charges within the 6 months immediately preceding or following the date of that call. This defined, relatively short window ensures that any identified criminal justice involvement is temporally proximate to the mental health episode, reflecting immediate pre- or post-incident system contact.
To accurately analyze the intersection of mental health crises and criminal justice involvement, a critical challenge involved isolating the specific individual experiencing the crisis from all other persons documented in the incident. Police services often house occurrence (UCR coded) and person data separately; therefore, the 1,414 mental health-related UCR calls were merged with the Barrie Police Service’s person data to identify the full cohort of individuals involved in these incidents. Within the Niche RMS, where person data are housed, there are multiple labels or classifications that can be assigned to an individual. For calls involving an individual experiencing a mental health crisis, the assigned person classification would be “person in crisis.” Alternatively, if the individual was apprehended by police, their classification would be “apprehended.” However, the resulting person dataset includes all parties involved in these calls, such as witnesses, complainants, and business owners. This is additionally challenged by the “dirty” nature of data in police records, where classifications are prone to subjectivity and error. For example, individuals may be classified as “subject of complaint” rather than “person in crisis.” Therefore, to attempt to gain the most accurate data of individuals subject to a mental health crisis during a mental health call, a wider range of person classifications needed to be considered.
Person classifications examined to narrow the data down in order to identify subjects of mental health crises in these calls were accused, adult accused diverted, apprehended, arrested, charged, subject of complaint, suicidal, deceased, located, person in crisis, person of interest, and person well-being check. Classifications deemed administrative or peripheral to the incident (e.g., attending physician, canvassed, child protection worker, complainant, landlord, parent/guardian, witness, vehicle owner) were excluded to focus the analysis on persons directly impacted or at the centre of the mental health event. However, it should be noted that there are limitations with this approach. Removing individuals from the person dataset based on their classification may also result in the removal of entire occurrences. This is particularly the case when only one person is involved and that person is not labelled as accurately as possible, for example, as a complainant only or as “other.” This reflects a limitation of the data and highlights the impact of labelling errors in operational police records.
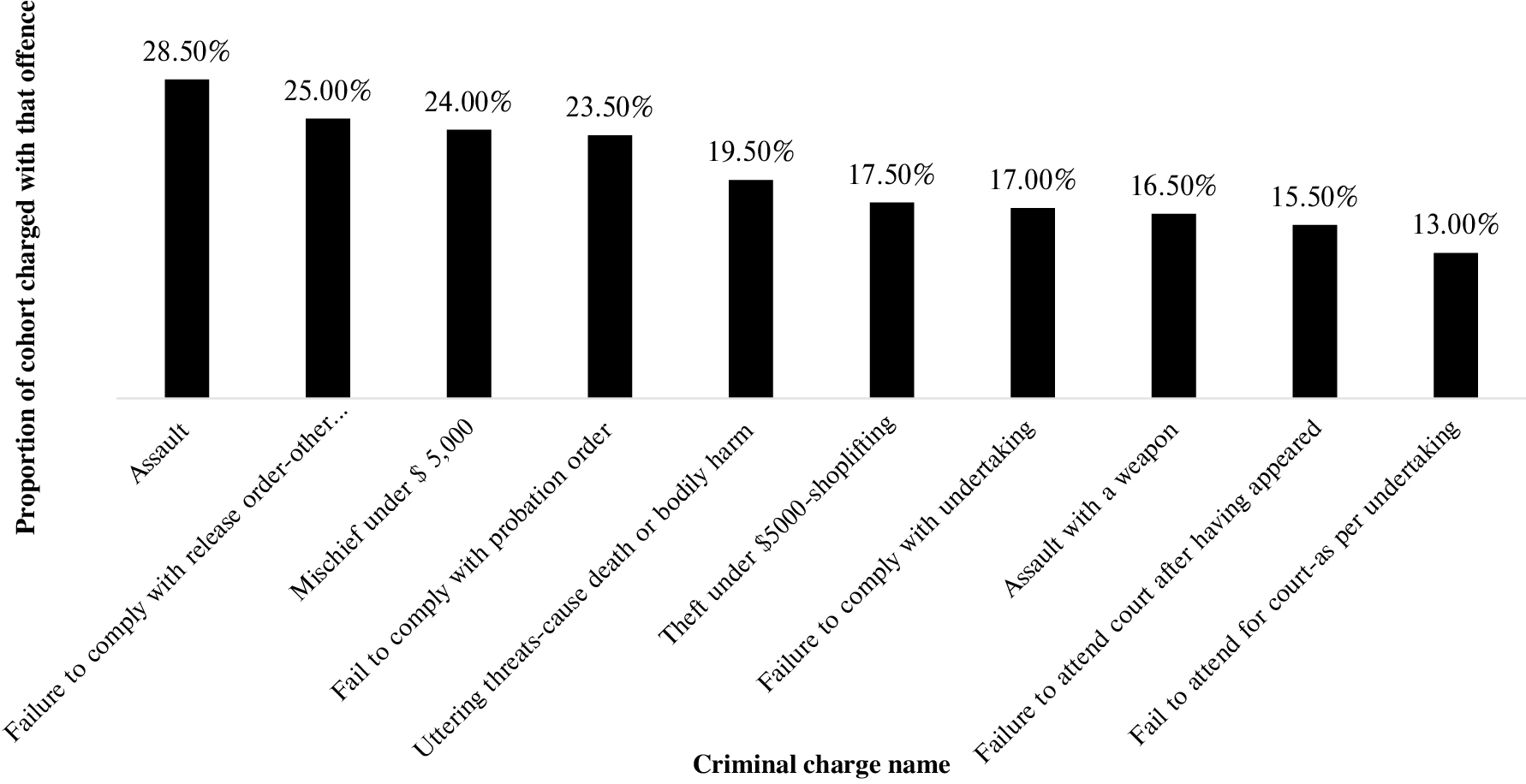
After applying these criteria, 759 unique individuals were identified as the person in crisis across 943 calls. While this number reflects a conservative estimate, it offers the most accurate snapshot possible given current data constraints. This removed 33% (n = 471) of mental health calls from the analysis, again showing the difficulty of isolating this information in police operational data. These person data were then connected to Barrie Police Service charged person data using a unique identifier to determine whether they had been criminally charged before or after their involvement in a mental health-related call. Focusing on temporal proximity to MHA involvement, we used each individual’s first MHA-coded occurrence in 2024 as a reference point. We examined their criminal charge history in the 6 months prior to and 6 months following their first mental health call in 2024. Therefore, the data range is from 1 July 2023 to 1 July 2025. Out of the 759 unique individuals who were the subject of mental health-related calls in 2024, 26% (n = 200) were criminally charged at some point during this 24-month window. To assess the temporal proximity of criminal involvement, charges were examined within the 6 months before and after an individual’s first 2024 mental health occurrence. These two groups are not mutually exclusive, meaning an individual may appear in both categories. Specifically, we found that 144 individuals (19%) were criminally charged in the 6 months prior to their first 2024 mental health occurrence. Alternatively, 103 individuals (14%) were criminally charged in the 6 months following that occurrence. The most common charge types among these 200 individuals were assault-related offences, failure-to-comply charges, mischief, and theft-related offences (see Figure 3).
|
|
||
|
FIGURE 3 Criminal charges attributed to subjects of mental health calls (2024). | ||
This study aimed to provide a comprehensive, data-driven analysis of mental health-related calls for service to the Barrie Police Service to inform the feasibility and necessity of implementing non-police, health-led alternative response models.
The analysis of call volume (RQ1) showed a gradual and consistent increase in mental health-related police responses over time, although this linear trend did not reach statistical significance. This pattern suggests a sustained or rising demand for police involvement that may be influenced by factors such as enhanced officer recognition, improved data coding, or societal stress, particularly in the aftermath of the COVID-19 pandemic. Also, given the lack of statistical significance, the variation might be purely due to chance. More critically, the analysis of call coding (RQ2) suggests a misalignment between initial risk perception and final documentation. Calls for service are categorized in real time by dispatchers based on information provided by the public (as detailed in the CAD data section). These findings (presented in Figure 4) suggest that many mental health-related calls are not always initially identified as such at the dispatch level. This indicates a potential gap between how the public describes a crisis and how communicators interpret it, compared to how the event is later documented by officers upon investigation. Additionally, this aligns with Ratcliffe’s (2021) findings in Philadelphia, noting the ambiguity and overlap between public health concerns and policing matters at the dispatch stage. This fundamental misalignment has direct implications for the appropriateness and effectiveness of the initial police response and may hinder the ability to appropriately allocate calls to non-police response teams.
|
|
||
|
FIGURE 4 Initial call classification codes of mental health Uniform Crime Reporting data (2024). | ||
The findings from RQ3 are arguably the most compelling rationale for expanding diversion strategies. The data reveal that in the majority of incidents, police responded to mental health-related calls that did not result in criminal charges or require law enforcement authority. While police presence may remain justified in high-risk or violent scenarios, many calls fell outside this extreme. Additionally, in the 1.27% of calls that resulted in charges, they tended to be lower-level offences such as mischief, failure to comply with past release orders, minor assault, and uttering threats. This demonstrates that these incidents do not often end in criminal charges related to violence or harm against individuals. These data, while an isolated case study, demonstrate that these calls are often low risk for public safety threats and can be handled appropriately by a non-police team.
Furthermore, the person-level analysis revealed that only 26% (n = 200) of individuals involved in MHA-coded calls had been criminally charged within a 6-month window before or after the incident. Even among this subset, the charges similarly reflect those above: assault level 1, failure to comply, mischief, and threats. It is crucial to understand that further police involvement does not imply a direct causal link between a mental health call and subsequent criminal charges. Rather, the initial contact introduces an individual into a criminal justice system that is fundamentally ill-equipped to provide appropriate mental health and social support (Schneider, 2015; Theuer, 2024). Consequently, they are more likely to accrue later charges, such as “failure to comply,” which often stem from missed administrative obligations related to probation or court orders, or public order offences like “mischief” or “trespass” driven by related issues like poverty and homelessness (Vogel et al., 2014). The prevalence of these charges, even in this subset of individuals, ultimately reflects a failure of pre-arrest diversion and community care infrastructure, turning a health issue into a perpetual cycle of criminal justice involvement.
This finding aligns with past research that has noted that individuals with mental illnesses are overrepresented in the criminal justice system mainly due to a high rate of low-level, non-violent arrests often related to nuisance behaviour, homelessness, or survival-related crimes (e.g., petty theft/property crime). Literature additionally notes that this is often compounded further through co-occurring substance use disorders (Steadman & Naples, 2005; Vogel et al., 2014). These data refute the fear regarding the criminal risk posed by this population, demonstrating that their involvement in serious, violent crime is limited. Furthermore, for those rare instances where police are required, the existing direct line of communication with dispatchers allows for rapid deployment of backup. Additionally, this challenges the narrative often told that people with mental health challenges are violent and unpredictable (Canadian Mental Health Association, 2011). While there is a gap in Ontario-specific research on violence and mental health, this study aims to demonstrate that in this specific context, mental health calls rarely end in criminal charges, and the subjects of these calls rarely engage in violent criminal activity.
Collectively, these findings offer a robust argument for immediately scaling alternative response models. Non-police, health professional-led teams or co-response models provide a more targeted, compassionate, and therapeutic approach to crisis intervention. Not only would this improve care, but it would also strategically reduce the burden on police resources and boost system efficiency by diverting a significant amount of these calls away from front-line police response (Burton et al., 2024; Davis et al., 2025; Gillespie et al., 2024). For example, Denver’s STAR program evaluation demonstrated that in its beginning years, the team only required co-response with other emergency agencies (such as police and paramedics) 13% of the time (Gillespie et al., 2024). Additionally, CAHOOTS’ evaluation discusses the cost savings of a non-police response team through significant hourly wage savings, from nearly $47 per hour for police to $18 per hour for a CAHOOTS response (Davis et al., 2025). This is important, as these programs show positive outcomes, an uptick in adoption, better social service navigation and cost savings (Davis et al., 2025). This study confirms that while police backup must remain an option, a traditional law enforcement response should be treated as the exception, reserving it for truly high-risk scenarios, rather than the automatic default. Finally, the power-law distribution, as well as the small concentration of charges and individuals arrested pre- and post-arrest, helps identify a specific cohort that could perhaps benefit from better service navigation and mental health resources immediately.
This study provides an important data-driven view of mental health calls but is subject to several limitations inherent to retrospective research utilizing administrative data. First, the analysis is dependent on administrative police data (CAD and UCR) which, as highlighted in the Methods section, is subject to human error and subjective coding practices. This introduces a risk of “dirty data” and may lead to either an underestimation of true mental health crises (due to miscoding) or an overestimation of police-recorded incidents (due to the subjective nature of initial dispatch categorization). This is particularly salient when attempting to isolate the individuals at the centre of mental health calls, resulting in an exclusion of 33% of call data. Second, as an observational, retrospective study, it cannot establish causal relationships. While a correlation between mental health contact and subsequent criminal charges is identified, this study cannot determine whether police contact itself contributed to further entanglement (e.g., through conditional release orders leading to failure-to-comply charges) or if the charges were independent of the crisis call. Third, the scope of the data is limited to a single, mid-sized Canadian police service. Caution must be exercised when attempting to generalize these specific findings regarding call volume, proportions, and criminal involvement profiles to larger, more densely populated metropolitan jurisdictions or to differing legal frameworks across regions. Finally, the study lacks underlying clinical data. Information regarding the individuals’ diagnosis, severity of illness, or treatment history is unavailable, limiting the ability to fully contextualize the clinical needs of the cohort and refine recommendations for clinical support models.
The author wishes to acknowledge Samantha Scott and Chief Rich Johnston for their valuable contributions.
None.
The author has no conflicts of interest to declare.
None.
None.
∗Barrie Police Service, Barrie, ON, Canada.
Addison, H., Shefner, R., Wood, J., & Anderson, E. (2023). Resident perspectives on police involvement in the response to mental health crises. Journal of Community Safety & Well-Being, 8(3), 112–118. https://doi.org/10.35502/jcswb.322
Ahonen, L., Loeber, R., & Brent, D. A. (2019). The association between serious mental health problems and violence: Some common assumptions and misconceptions. Trauma, Violence, & Abuse, 20(5), 613–625. https://doi.org/10.1177/1524838017726423
Atherley, L. T. (2025). Risk managed demand: Operational risk management in police response to calls for service. Police Quarterly. https://doi.org/10.1177/10986111251383548
Barrie Police Service. (2025). 2024 Annual Report. https://www.barriepolice.ca/newsroom/publications/
Boyce, J., Rotenberg, C., & Karam, M. (2015). Mental health and contact with police in Canada, 2012. Juristat: Canadian Centre for Justice Statistics, 1, 3–25.
Burton, N., Herbert, C., & Rohlfs, R. (2024). Quantifying CAHOOTS: Mobile crisis response program diverts and prevents police. Public Health, 24, 2183.
Canadian Mental Health Association Ontario. (2011). Violence and mental health: Unpacking a complex issue. https://ontario.cmha.ca/documents/violence-and-mental-health-unpacking-a-complex-issue/
Centre for Addiction and Mental Health. (2023). Toronto Community Crisis Service: Outcome evaluation report.
City of Denver. (n.d.). Support Team Assisted Response (STAR) program. https://www.denvergov.org/Government/Agencies-Departments-Offices/Agencies-Departments-Offices-Directory/Public-Health-Environment/Community-Behavioral-Health/Behavioral-Health-Strategies/Support-Team-Assisted-Response-STAR-Program
City of Durham. (n.d.). 911 Crisis response (HEART). https://www.durhamnc.gov/5461/911-Crisis-Response-HEART#:~:text=Community%20Response%20Teams%20provide%20rapid,unarmed%2C%20skilled%20and%20compassionate%20first
City of Eugene. (2025). Mobile Crisis Services. https://www.eugene-or.gov/5389/Mobile-Crisis-Services
City of Toronto. (n.d.). Toronto Community Crisis Service. https://www.toronto.ca/community-people/public-safety-alerts/community-safety-wellbeing-programs/toronto-community-crisis-service/
Choe, J. Y., Teplin, L. A., & Abram, K. M. (2008). Perpetration of violence, violent victimization, and severe mental illness: Balancing public health concerns. Psychiatric Services, 59(2), 153–164. https://doi.org/10.1176/ps.2008.59.2.153
Coleman, T. G., & Cotton, D. (2016). A strategic approach to police interactions with people with a mental illness. Journal of Community Safety and Well-Being, 1(2), 7–11. https://doi.org/10.35502/jcswb.9
Cotton, D., & Coleman, T. G. (2014). Canadian police agencies and their interactions with persons with a mental illness: A systems approach. In Police responses to people with mental illnesses (pp. 13–26). Routledge.
Compton, M. T., Bakeman, R., Broussard, B., Hankerson-Dyson, D., Husbands, L., Krishan, S., Stewart-Hutto, T., D’Orio, B. M., Oliva, J. R., Thompson, N. J., & Watson, A. C. (2014). The police-based crisis intervention team (CIT) model: I. Effects on officers’ knowledge, attitudes, and skills. Psychiatric Services, 65(4), 517–522. https://doi.org/10.1176/appi.ps.201300107
Davis, J., Norris, S., Schmitt, J., Shem-Tov, Y., & Strickland, C. (2025). Mobile crisis response teams support better policing: Evidence from CAHOOTS. National Bureau of Economic Research.
Dempsey, C., Quanbeck, C., Bush, C., & Kruger, K. (2020). Decriminalizing mental illness: Specialized policing responses. CNS Spectrums, 25(2), 181–195. https://doi.org/10.1017/S1092852919001640
El-Sabawi, T., & Carroll, J. J. (2021). A model for defunding: An evidence-based statute for behavioral health crisis response. Temple Law Review, 94, 1.
Elbogen, E. B., & Johnson, S. C. (2009). The intricate link between violence and mental disorder. Archives of General Psychiatry, 66(2), 152. https://doi.org/10.1001/archgenpsychiatry.2008.537
Fahim, C., Semovski, V., & Younger, J. (2016). The Hamilton mobile crisis rapid response team: A first-responder mental health service. Psychiatric Services, 67(8), 929.
Gillespie, S., Curran-Groome, W., & Rogin, A. (2024). Evaluating alternative crisis response in Denver’s Support Team Assisted Response (STAR) program. Urban Institute.
Huey, L., Ferguson, L., & Vaughan, A. D. (2021). The limits of our knowledge: Tracking the size and scope of police involvement with persons with mental illness. Facets, 6(1), 424–448. https://doi.org/10.1139/facets-2021-0005
Lamb, H. R., Weinberger, L. E., & Gross, B. H. (2004). Mentally ill persons in the criminal justice system: Some perspectives. Psychiatric Quarterly, 75, 107–126. https://doi.org/10.1023/b:psaq.0000019753.63627.2c
Ratcliffe, J. H. (2021). Policing and public health calls for service in Philadelphia. Crime Science, 10(1), 5. https://doi.org/10.1186/s40163-021-00141-0
Schneider, R. D. (2015). The mentally ill: How they became enmeshed in the criminal justice system and how we might get them out. Department of Justice Canada.
Sinha, M. (2009). An investigation into the feasibility of collecting data on the involvement of adults and youth with mental health issues in the criminal justice system (Catalogue no. 85-561-M — No. 016; Crime and Justice Research Paper Series). Statistics Canada. www.statcan.gc.ca/pub/85-561-m/85-561-m2009016-eng.pdf
Shapiro, G. K., Cusi, A., Kirst, M., O’Campo, P., Nakhost, A., & Stergiopoulos, V. (2015). Co-responding police-mental health programs: A review. Administration and Policy in Mental Health and Mental Health Services Research, 42(5), 606–620. https://doi.org/10.1007/s10488-014-0594-9
Sherman, L. W. (2007). The power few: Experimental criminology and the reduction of harm. Journal of Experimental Criminology, 3(4), 299–321. https://doi.org/10.1007/s11292-007-9044-y
Statistics Canada. (2024). Census profile, 2021 census of population. https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/details/page.cfm?Lang=E&SearchText=barrie&DGUIDlist=2021A00053543042&GENDERlist=1,2,3&STATISTIClist=1&HEADERlist=0
Steadman, H. J., & Naples, M. (2005). Assessing the effectiveness of jail diversion programs for persons with serious mental illness and co-occurring substance use disorders. Behavioral Sciences & the Law, 23(2), 163–170. https://doi.org/10.1002/bsl.640
Theuer, A. (2024). Examining police, health, and mental health crisis response teams [Doctoral dissertation, McMaster University]. MacSphere. https://macsphere.mcmaster.ca/items/a61da9b4-1d75-4e47-9787-612bcebfae53.
Thompson, C. (2024, July 25). Sending unarmed responders instead of police: What we’ve learned. The Marshall Project. https://www.themarshallproject.org/2024/07/25/police-mental-health-alternative-911
Vogel, M., Stephens, K. D., & Siebels, D. (2014). Mental illness and the criminal justice system. Sociology Compass, 8(6), 627–638. https://doi.org/10.1111/soc4.12174
Wood, J., Swanson, J., Burris, S., & Gilbert, A. (2011). Police interventions with persons affected by mental illnesses: A critical review of global thinking and practice. Centre for Behavioural Health Services and Criminal Justice Research, Rutgers University.
Correspondence to: Madison Charman, 110 Fairview Road, Barrie, ON L4N 8X8, Canada. Telephone: 705-725-7025 ext. 2244. E-mail: mcharman@barriepolice.ca
This work is distributed under the Creative Commons BY-NC-ND license. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/. For commercial re-use, please contact sales@sgpublishing.ca.
Journal of CSWB, VOLUME 11, NUMBER 1, March 2026