SOCIAL INNOVATION NARRATIVE
Building a Wales without violence: Using behavioural science to implement a public health approach
Bryony Parry∗, Lara Snowdon∗,†, Emma R. Barton∗, Alex Walker∗, Joanne Hopkins∗, Alice Cline∗, Nicky Knowles∗
This article is related directly to the Seventh International Conference on Law Enforcement & Public Health (LEPH) held in Ottawa, Canada in July 2025.
ABSTRACT
Violence among children and young people is preventable through a public health approach. However, there remains a scarcity of knowledge about its implementation to effect system-level change for violence prevention and the range of public health actions available to support it. This article describes how the Wales Violence Prevention Team (VPT), Public Health Wales, applied behavioural science to inform the implementation of Wales Without Violence – a co-produced framework for preventing violence among children and young people. Using the capability, opportunity, motivation, behaviour model, the VPT engaged professionals across sectors to identify the behaviours, barriers, and facilitators for embedding the framework’s nine violence prevention principles. The process enabled an exploration of the support needed to enhance professionals’ capability, opportunity, and motivation for adopting a public health approach to violence prevention. The application of behavioural science to explore barriers and support needs for professionals involved in violence prevention also supported the VPT in clarifying its own role within the violence prevention landscape in Wales to maximize its resources. This article provides insights for advancing violence prevention activity through a public health approach.
Key Words Violence prevention; public health approach; behavioural science; COM-B model.
INTRODUCTION
Violence is preventable, and ending violence is possible. This message underlies the creation of Wales Without Violence: A shared framework for preventing violence among children and young people (the framework) (Snowdon et al., 2023). The framework outlines the key elements needed to successfully develop primary prevention and early intervention strategies to end violence among children and young people through a public health, whole-system approach. Co-produced between children, young people, and professionals, it is built on the foundations of national policy and legislation that support prevention and early intervention, including the Serious Violence Duty, which places a duty on public services across England and Wales to work together to prevent and reduce violence (Home Office, 2022), and the Violence Against Women, Domestic Abuse and Sexual Violence (Wales) Act (2015), which exists to improve arrangements for the prevention of and response to gender-based violence (Welsh Government, 2015). Together, this legislative context facilitates an environment that can prioritize violence prevention. This article presents how the Wales Violence Prevention Team (VPT) developed a behaviourally informed implementation plan for the Wales Without Violence Framework to support the implementation of a public health approach to violence prevention. This unique approach aimed to identify the support professionals need to adopt and maintain the behaviours necessary for a public health approach to violence prevention.
BACKGROUND
A Public Health Approach to Violence Prevention
Violence causes harm and compromises the safety and well-being of individuals, families, and communities. Violence disproportionally affects children and young people, with its impacts felt most acutely by those facing further structural inequalities (Snowdon et al., 2023). However, traditional responses to violence often focus on reactive or punitive measures when violence has already taken place rather than prevention (Krug et al., 2002). A public health approach conceptualizes violence as a population health issue which requires a systemic and multi-sectoral approach to reducing inequalities and promoting health and well-being. It utilizes data and multi-disciplinary evidence to improve knowledge and understanding of violence and to generate preventative, long-term solutions (Krug et al., 2002).
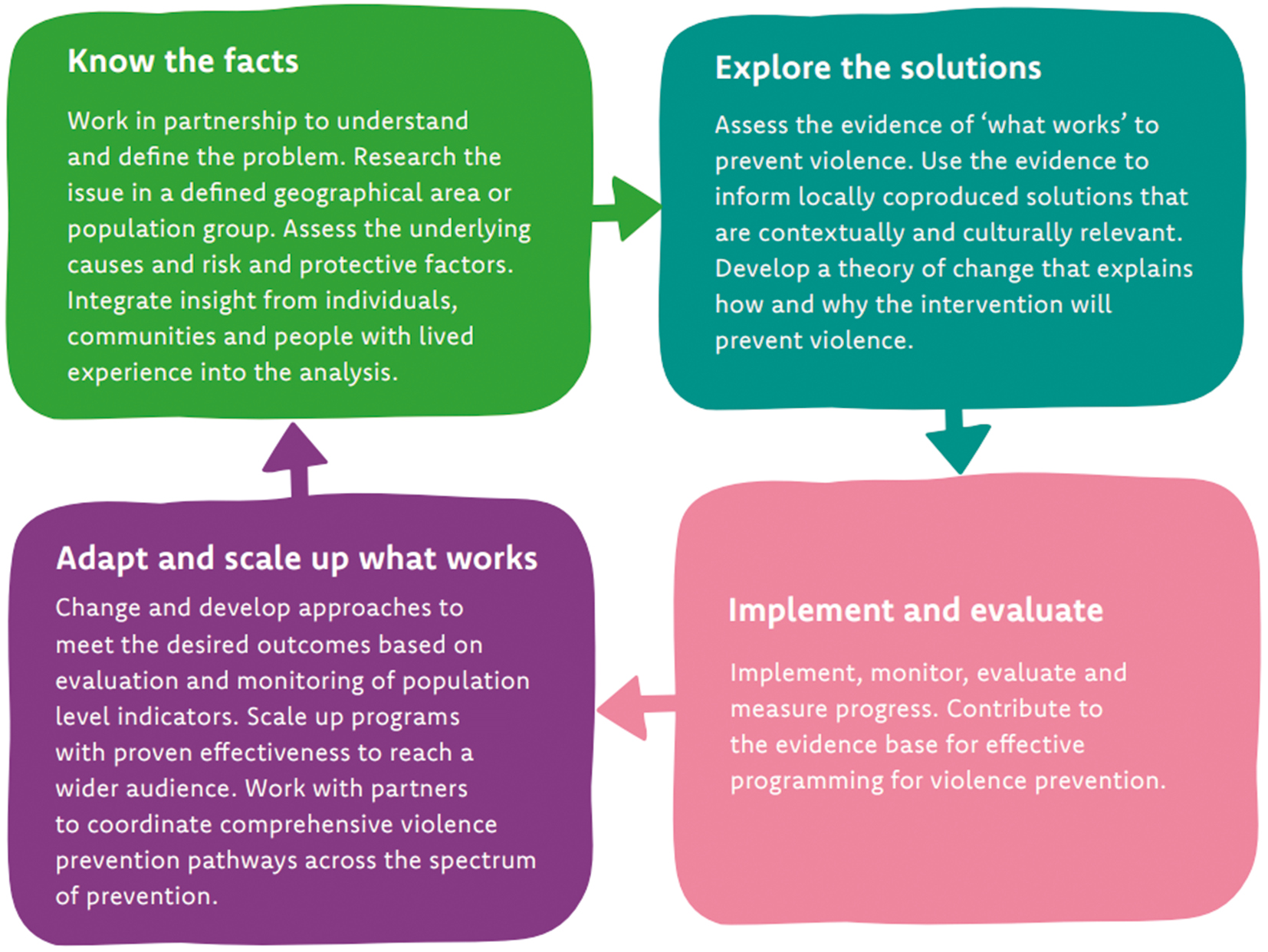
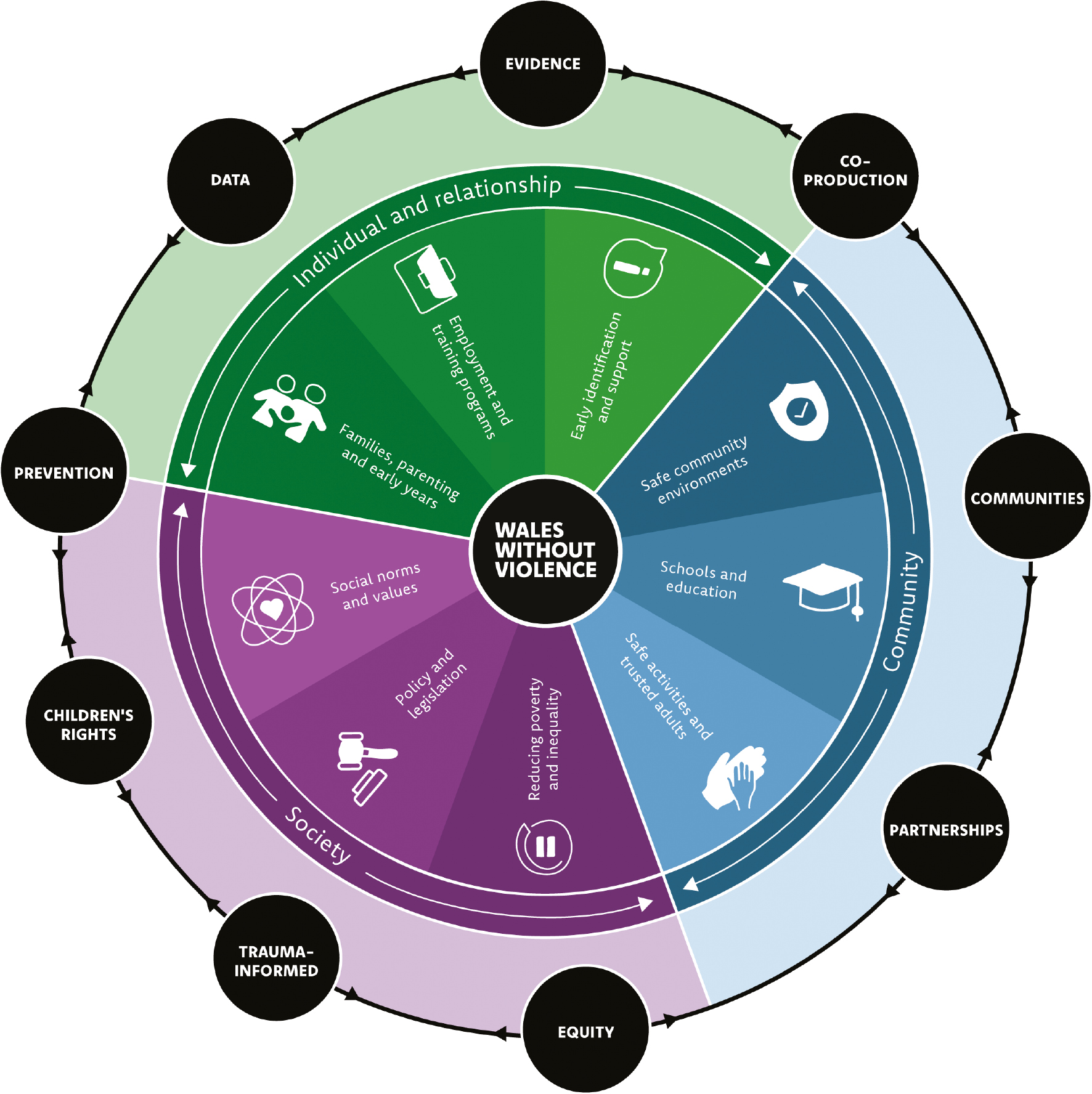
The framework is a guide for utilizing a public health approach for violence prevention, including an adapted version of the World Health Organization’s (WHO) four-step model for implementing a public health approach to violence prevention (Figure 1). The framework offers nine evidence-informed violence prevention strategies and nine co-developed principles to prevent violence across the life course and across individual, community, and societal contexts (Figure 2). The nine strategies articulate what interventions should be delivered to prevent violence, whilst the nine violence prevention principles, identified by children, young people, and professionals, set out how activity should be delivered. Taken together, the strategies and the principles seek to ensure primary prevention and early intervention can be prioritized at the individual, community and societal levels and that violence prevention activity is coordinated with and aligned to key practices and approaches.
|
|
|
FIGURE 1 The four stages of a public health approach to violence prevention (Snowdon et al., 2023). Adapted from the World Health Organization’s four-step model for implementing a public health approach to violence prevention, this model reflects the views of stakeholders in Wales and the developments in knowledge about the practical implementation of violence prevention efforts. |
|
|
|
FIGURE 2 Strategies and principles for a Wales without violence (Snowdon et al., 2025). This infographic demonstrates how the nine violence prevention strategies included in the framework, which form the centre circle, can be mapped against the socio-ecological model to ensure that primary prevention and early intervention are prioritized at the individual, community, and societal levels. The principles that are identified in the outer circles support and inform the delivery of the strategies so that violence prevention activity is coordinated with and aligned to key practices and approaches. |
Whilst the framework provides insight into a public health approach within the context of violence prevention, there is a scarcity of global evidence on effective implementation, with limited studies reporting on the barriers of embedding this approach (Snowdon et al., 2024). Therefore, to embed the framework, and thereby a public health approach, in professional practice, it is critical to understand the challenges and opportunities faced by professionals seeking to implement a public health approach to violence prevention.
Behavioural Science for Public Health
Behavioural science is increasingly used to explore health behaviours, understand their influences, and explore how best to address them, which is essential to achieving positive public health policy and practice outcomes (Knowles & Gould, 2023). More broadly, behaviour change models and frameworks enable the identification of evidence-informed strategies for influencing behaviours to achieve desired outcomes, which is important when seeking to understand and evolve professional practice, as was necessary for the implementation of the Wales Without Violence Framework.
The capability, opportunity, motivation, behaviour (COM-B) model (Michie et al., 2011) provides a framework for exploring the determinants of behaviours. Within the COM-B model, “capability” is defined as the individual’s psychological and physical capacity to engage in a behaviour. “Motivation” includes goals and analytical decision-making – things we are overtly aware of – as well as more subconscious processes like our habits, values, and emotional responses. “Opportunity” is defined as all the factors that lie outside the individual that make the behaviour possible or prompt it (Michie et al., 2011). The VPT recognized that by utilizing the COM-B model, they would be able to explore the behaviours that underpin each of the nine violence prevention principles, which are intended to articulate what a public health approach means in practice. This activity would enable an investigation of the drivers (barriers or facilitators for achieving the desired behaviour) of professional behaviours to support the identification of evidence-informed behaviour change strategies, with the aim of eliciting and maintaining the behaviours that underpin a public health approach.
TRANSLATING PRINCIPLES INTO PRACTICE
The VPT ran engagement sessions with professionals to investigate participants’ experience and perceptions of adopting the nine violence prevention principles against the COM-B model (Michie et al., 2011). The engagement sessions first focused on establishing the behaviours needed to achieve the nine violence prevention principles before identifying their drivers. Through this process, the team aimed to develop a shared understanding of what a public health approach means in practice for professionals in Wales, as well as better explore the support needed to enable a public health approach to violence prevention, by identifying evidence-informed behaviour change strategies for implementing the framework.
Engagement Design and Delivery
The VPT conducted a two-part engagement series with 65 professionals from policing, health, education, government, local authorities, and the third sector. The VPT invited professionals who had signed up to the team’s mailing list, and upon registration, participants were asked to rank the nine violence prevention principles in terms of interest and perceived relevance to their role. During the sign-up process, participants were also asked to confirm their attendance for both sessions, as the series design meant that session 2’s exploration of behavioural drivers was founded on the ideas and professional opinion of behaviours established in the first session. Therefore, it was important that the same professionals were in attendance for both events.
The VPT collaborated with the Behavioural Science Unit (BSU), Public Health Wales, on the design and delivery of the engagement events. The BSU provides specialist expertise on behavioural science and champions and enables the increasingly routine application of it to improve health and well-being in Wales (Behavioural Science Unit, 2024). In session 1, the VPT provided an overview of the framework, including the nine violence prevention principles, and the BSU introduced the key concepts of behavioural science and defined what constitutes a behaviour. Participants were then divided into three breakout groups according to the ranking exercise completed upon their registration to discuss behaviours related to three of the violence prevention principles. Each group was facilitated by a VPT team member who had specific expertise in the principles being discussed. An additional member of the VPT team took notes of the breakout discussions in real time on a shared, collaborative whiteboard platform, so participants had an opportunity to query or clarify the discussion. The breakout sessions resulted in the identification of a total of 117 behaviours. These were later synthesized into three core behaviours for each of the nine principles by the VPT, which were shared with participants to review.
Session 2 comprised a discussion about the core behaviours established from session 1 and a guided exploration of the COM-B model (Michie et al., 2011) led by the BSU. A second breakout session was dedicated to conducting a collaborative behavioural diagnosis for each of the core behaviours using the COM-B model. To prompt and guide discussion, a series of agreed framing questions was provided by breakout session facilitators. These questions were taken from a guide on collecting behavioural insights (Cline et al., 2023) and aimed to elicit capability drivers (e.g., “How well do they know how to do it?”), opportunity drivers (e.g., “How far is it considered ‘normal’ within the social environment?”), and motivation drivers (e.g., “How worthwhile do they think it is?”). Following session 2, the VPT mapped the barriers and facilitators onto the COM-B model. This resulted in three COM-B models for each principle, which were then synthesized into one overarching COM-B model for each principle.
SELECTING APPROPRIATE INTERVENTION AND IMPLEMENTATION OPTIONS
The professional insight gathered through the engagement events enabled the VPT to explore effective interventions and implementation strategies to increase the likelihood of the adoption of a public health approach by violence prevention professionals. The team followed guidance on behaviour change techniques (Cline et al., 2024) and used the Behaviour Change Technique Taxonomy (Michie et al., 2013), leading to the design of a “behaviour and action map.” The map attaches an appropriate mechanism of action and behaviour change technique to each of the behavioural barriers, enabling the VPT to consider the most effective action it could take to elicit professional behaviour change. This process drew on behaviour change theory, professional insight, and the VPT’s knowledge of their own existing and anticipated resource capabilities to develop a pragmatic and participatory-led approach to supporting partners in implementing the Wales Without Violence Framework.
KEY FINDINGS: COMMON REPORTED BEHAVIOURS AND BARRIERS TO ADDRESS
The VPT conducted a thematic analysis of the behaviours, barriers, and facilitators identified by the participants for each of the nine principles. This analysis has provided an understanding of what a public health approach looks like in practice, to better support the measurement and evaluation of the approach’s implementation, as well as actionable insight into the challenges and opportunities of implementing a public health approach to violence prevention.
Cross-Cutting Behaviours
Collecting and sharing data
Behaviours focused on sharing data, including utilizing systems that enabled multiple organizations to access the same data to enable joint decision-making, and on data collection, namely collecting data on protected characteristics to enable an intersectional analysis of violence.
Partnerships with people, communities, and professionals
Across principles, behaviours to demonstrate effective partnership working focused on communication skills, developing processes and policies in relation to partnerships and involvement, and utilizing culturally competent engagement methods.
Collaboration
Primarily, participants identified that collaboration behaviours focused on enabling active participation of diverse groups, building governance structures to formalize collaboration opportunities, and developing processes that enable an understanding of and response to the needs of staff participating in partnerships.
Funding
Specifically, principles highlighted that professionals should proactively resource prevention activities, for example, by including co-production in budget planning or allocating budget and resources to integrate prevention initiatives into existing services such as healthcare provision.
Cross-Cutting Barriers and Facilitators
Knowledge, awareness, and skills
Across all discussions, there was a perceived lack of knowledge, awareness, and skills needed to embody the behaviours that represent each of the principles. Participants articulated a lack of knowledge about data sharing and collection policies, how to design and deliver evaluation, and what certain terminology means, for example, the terms “trauma informed,” “a whole-system approach,” and “intersectionality.” There was a lack of awareness about what services and partnership arrangements already existed and a perceived lack of skill in engaging with diverse communities, co-production, and conducting research and evaluation to inform activity.
Processes and systems
Participants raised that there were inadequate processes and systems in place to enable a public health approach to violence prevention. Processes that were seen to act as a barrier to eliciting the behaviours included differing data sharing policies across organizations and governance processes that deter participation from marginalized groups. Participants also highlighted barriers relating to incompatible information technology systems that hindered cross-organizational working and a lack of standardized training.
Capacity and resources
Within this theme sits barriers like time, role duties and responsibilities, and technology. Barriers relating to this theme were apparent in all nine principles. Barriers included a lack of time to build the relationships necessary for effective co-production and involvement, a lack of time to attend partnership meetings, high staff turnover, a lack of funding, a lack of sustainable funding, a lack of capacity in services, an unequal distribution of services across the country, and no time to dedicate to evaluating services.
Norms and confidence
Several participants identified that current norms were not conducive to implementing a public health approach to violence prevention. Barriers focused on norms related to a lack of “buy-in” or recognition of the strengths of the approach which resulted in difficulty when trying to evolve standard practice. Participants reported a lack of confidence at both the individual and organizational level in carrying out behaviours related to co-production, using an intersectional approach, data collection and sharing, and evaluation.
UNDERSTANDING AND COMMUNICATING OUR ROLE IN SYSTEM CHANGE: THE RISE APPROACH
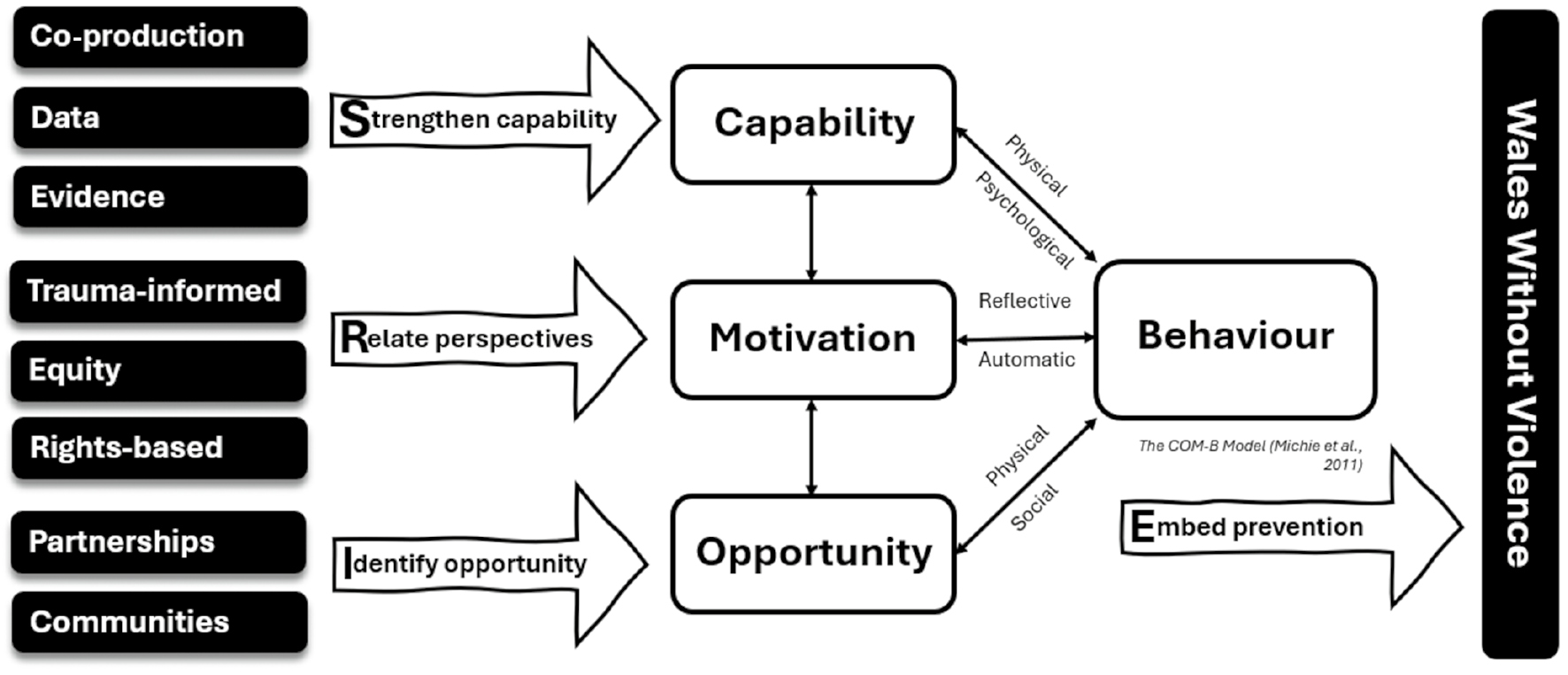
To support the prioritization of actions within the “behaviour and action map” and to enable the VPT to outline to professionals how they will work with them to embed the framework into practice, the VPT developed the RISE (relate perspectives, identify opportunity, strengthen capability, embed prevention) approach (Figure 3). This approach outlines the tiered system of support that the VPT will offer professionals for each of the nine violence prevention principles. The tiers range from technical support aimed to increasing knowledge and improving skills to strengthening and supporting the infrastructure needed for violence prevention and finally ensuring aligned approaches and strategies are coordinated within and across the violence prevention landscape to achieve the aim of embedding a public health approach to violence prevention.
|
|
|
FIGURE 3 The RISE approach mapped onto the COM-B model. The RISE approach was developed by the Violence Prevention Team, Public Health Wales, through their application of behavioural science for the implementation of a public health approach. It outlines the tiered system of support they will provide professionals in embedding the nine violence prevention principles, in line with the behavioural domains of the COM-B model (Michie et al., 2011). The tiers range from technical support aimed at increasing knowledge and improving skills to strengthening and supporting the infrastructure needed for violence prevention and finally ensuring that aligned approaches and strategies are coordinated within and across the violence prevention landscape to achieve the ultimate aim of embedding a public health approach to violence prevention. COM-B, capability, opportunity, motivation, behaviour model; RISE, relate perspectives, identify opportunity, strengthen capability, embed prevention approach. |
Relate Perspectives
As part of the implementation of the Wales Without Violence Framework, the VPT will promote trauma-informed, equitable, and rights-based approaches by sharing information, raising awareness, and improving coordination across sectors.
Identify Opportunity
The VPT will support participation and strengthen partnerships for prevention by contributing expertise and enabling community-based, collaborative working.
Strengthen Capability
The VPT will build capacity to deliver a public health approach through co-production, data analysis, and evidence-based practice by providing technical support, resources, and skills development opportunities.
Embed Prevention
The activity delivered by the VPT, developed in response to professional insight into the challenges of implementing a public health approach, seeks to ensure partners have the capability, opportunity, and motivation to implement this approach, which will in turn drive long-term, system-wide change toward a Wales Without Violence.
REFLECTIONS
Whilst there is increasing evidence of using behavioural science to explore and address health behaviours (Knowles & Gould, 2023), this was an innovative approach taken by the VPT and BSU to explore how behavioural science could be applied to the prevention of violence as part of a public health approach. Our investigation into the range of professional behaviours related to violence prevention implementation, and the barriers and support needs of professionals in achieving these, has yielded new insight into how behavioural science can be applied to support both individual and system change. It also generates new insight into the range of actions available to a public health team in supporting system change for a public health approach to violence prevention.
As a new approach, it is essential that it is evaluated to understand the process of implementation and outcomes. The VPT discovered that the process itself lays the foundations necessary for evaluation. Understanding behavioural drivers and identifying specific actions to elicit a desired behaviour improved the VPT’s ability to develop outputs and anticipated outcomes to support the development of a theory of change and measures for evaluation.
The approach engaged a diverse professional audience and generated actionable insights to support the implementation of a public health approach to violence prevention. However, there was a variability in participation across the sessions which affected the consistency of input. Future work should ensure consistent engagement and consider segmenting participants by professional groups to gain a thorough understanding of the barriers facing each profession. It was important that the subject matter expertise held by the VPT was combined with expertise from the BSU on behavioural science to maximize input from professionals and to identify the potential range of actions.
CONCLUSION
Applying behavioural science to understand the influences on professional behaviours needed for violence prevention offers an innovative and practical pathway for investigating the support required for the implementation of a public health approach. The application of behaviour theory and behaviour change models helps translate a public health approach into measurable behaviours and associated barriers that can guide the development of practices supportive of the approach.
ACKNOWLEDGEMENTS
We appreciate the honest and insightful involvement of all those who participated in the events outlined in this narrative. We thank Muqaddasa Abdul Wahid and Shauna Pike, who provided much-valued facilitation and documentation support for the events.
CONFLICT OF INTEREST DISCLOSURES
The authors have no conflicts of interest to declare.
AUTHOR AFFILIATIONS
∗Policy and International Health, WHO Collaborating Centre on Investment for Health and Well-being, Public Health Wales, Cardiff, UK;
†World Health Organization Collaborating Centre for Violence Prevention, Public Health Institute, Liverpool John Moores University, Liverpool, UK.
REFERENCES
Behavioural Science Unit. (2024). About us. Public Health Wales World Health Organization Collaborating Centre on Investment for Health and Well-being. https://phwwhocc.co.uk/bsu/about-us/
Cline, A., Gould, A., & West, J. (2023). Behavioural diagnosis: How to collect behavioural insights. Public Health Wales. https://phwwhocc.co.uk/wp-content/uploads/2023/06/Behavioural-Diagnosis-How-to-collect-behavioural-insights-v1d.pdf
Cline, A., Knowles, N., West, J., & Gould, A. (2024). Identifying and applying behaviour change techniques. Public Health Wales. https://phwwhocc.co.uk/wp-content/uploads/2024/02/Identifying-and-Applying-Behaviour-Change-Techniques-1.pdf
Home Office. (2022). Serious Violence Duty. https://www.gov.uk/government/publications/serious-violence-duty
Knowles, N., & Gould, A. (2023). Exploring factors influencing the application of behavioural science within public health practice across Wales. Public Health Wales. https://phwwhocc.co.uk/wp-content/uploads/2023/06/Capability-and-Readiness-Report-V1c-1.pdf
Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B., & Lozano, R. (2002). World report on violence and health. World Health Organization.
Michie, S., van Stralen, M. M. & West, R. (2011). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 6, 42. https://doi.org/10.1186/1748-5908-6-42
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J., & Wood, C. E. (2013). The Behavior Change Technique Taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6
Snowdon, L., Parry, B., Walker, A., & Barton, E. (2023). Wales Without Violence: A shared framework for preventing violence among children and young people. Public Health Wales. https://waleswithoutviolence.com/wp-content/uploads/2023/04/WWV-Framework-Digital-English.pdf
Snowdon, L., Quigg, Z., & Leavey, C. (2024). The role of public health in the primary prevention of interpersonal violence: A systematic review of international frameworks. Journal of Community Safety and Well-Being, 9(4), 176–183. https://doi.org/10.35502/jcswb.406
Snowdon, L., Parry, B., & Barton, E. (2025). Wales Without Violence: A shared framework for preventing violence among children and young people - infographic. Public Health Wales. https://waleswithoutviolence.com/the-framework/infographic-building-a-wales-without-violence/
Welsh Government. (2015). Violence Against Women, Domestic Abuse and Sexual Violence (Wales) Act. https://www.legislation.gov.uk/anaw/2015/3/contents
Correspondence to: Bryony Parry, Public Health Wales, 2 Capital Quarter, Tyndall Street, Cardiff CF10 4BZ, UK. E-mail: bryony.parry@wales.nhs.uk
(Return to Top)
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/. For commercial re-use, please contact sales@sgpublishing.ca.
Journal of CSWB, VOLUME 10, NUMBER 4, December 2025